How We Treat Benign Esophageal Disease?

Treatment of benign esophageal disease involves a multidisciplinary approach and may include lifestyle modifications, medications, endoscopic interventions, surgical procedures, surveillance, and management of high-grade dysplasia.
The gastrointestinal team at Saint John’s is highly experienced, treating thousands of patients each year. These specialists include GI surgeons, medical oncologists, and radiation oncologists, as well as on-site pathologists, geneticists, nutritionists, and immunologists.
Working to Alleviate Symptoms
Benign esophageal diseases encompass a range of conditions affecting the esophagus, including gastroesophageal reflux disease (GERD), hiatal hernia, esophageal motility disorders, esophageal diverticula, esophageal strictures, eosinophilic esophagitis, and Barrett’s esophagus. Prompt diagnosis and appropriate treatment are crucial to alleviate symptoms, improve quality of life, and prevent complications.
In order to determine the best course of treatment, a proper diagnosis is conducted to rule out other health problems and diseases. Diagnosis of benign esophageal disease begins with a thorough patient history and physical examination. Diagnostic tests such as upper endoscopy, barium swallow, esophageal manometry, pH monitoring, and biopsy help determine the specific condition and guide treatment decisions.
How can diet and lifestyle changes improve esophageal conditions?
Lifestyle modifications play a significant role in managing benign esophageal diseases. These include dietary changes, weight loss, avoiding trigger foods, and elevating the head of the bed to reduce reflux. Medications such as proton pump inhibitors (PPIs), H2 receptor antagonists, antacids, and prokinetic agents are commonly used to alleviate symptoms and reduce acid production. In cases of eosinophilic esophagitis, topical steroids may be prescribed.
There are several lifestyle changes you can make to alleviate a variety of esophageal symptoms:
- Avoid lying flat for at least two hours after a eating or drinking acidic beverages, including beverages with high caffiene.
- If you are experiencing symptoms, keep your head and upper body somewhat elevated while you sleep. Using an extra pillow or two can help prevent reflux symptoms.
- Eat smaller and more frequent meals during the day instead of fewer larger meals. This helps improved digestion and reduce heartburn.
- Wear loose-fitting clothes around the stomach, excess pressure can worsen heartburn and reflux.
- Quit smoking. Smoking can increase the production of stomach acid and reduce the function of the lower esophageal sphincter. This muscle keeps acid and other stomach content from reentering the esophagus. Smoking can also decrease the amount of saliva that is produced in the mouth, which helps to neutralize acid produced by the body.
- Reduce excess weight around the midsection. By losing weight, stomach pressure is reduced. Such pressure can force some stomach contents back up the esophagus.
Endoscopic and Surgical Interventions
Endoscopic interventions are often employed to treat various conditions. Dilation of esophageal strictures can be achieved through endoscopic techniques, relieving swallowing difficulties. Endoscopic mucosal resection (EMR) and radiofrequency ablation (RFA) are employed for the management of Barrett’s esophagus, a condition associated with an increased risk of esophageal cancer. Endoscopic suturing can be used for repairing hiatal hernias, while stents are used for the management of esophageal perforations or leaks.
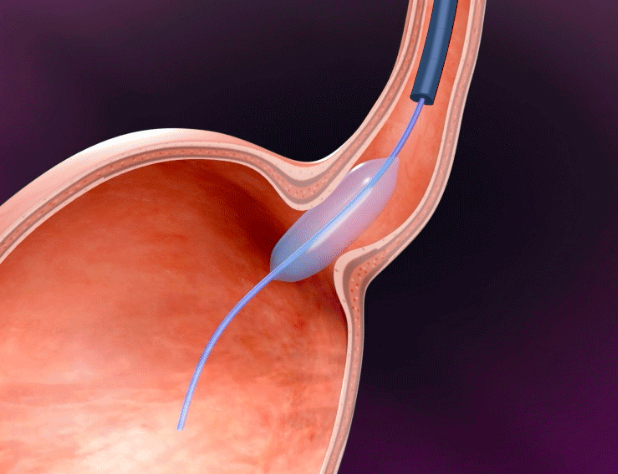
Dilation
Using Esophageal dilation (EGD), a catheter with a small balloon on the end is passed through the stricture. The balloon is slowly inflated to open the narrow area, which is referred to as balloon dilation. Other dilators may use flexible materials to expand the narrowing. The dilation process starts with smaller dilators and progressively increases in size. Most patients will experience relief after successful dilation. However, the recurrence rate after dilation is 30 to 40% within one year of treatment, even with the aid of concomitant acid suppression.
Surgery
Surgery is not the first line of treatment but may be necessary after medications and medical treatments such as dilation have failed. Surgery is reserved for cases where conservative measures and endoscopic treatments have also been ineffective. Fundoplication is a type of surgical procedure used to treat GERD. It reinforces the lower esophageal sphincter so that further damage to the esophagus from stomach acid is reduced.
If a hernia of the esophagus exists—a condition where part of the stomach can protrude into the chest cavity through a weak area of the diaphragm—Hiatal hernia repair surgery aims to reduce the herniated portion of the stomach into the chest. This surgery involves bringing the stomach down into the abdomen and making the opening in the diaphragm smaller or reconstructing an esophageal sphincter to prevent hernia.
Esophageal myotomy is a surgical procedure in which the muscles of the lower esophageal sphincter are modified, allowing food and liquids to pass to the stomach. This procedure is used to treat achalasia, a condition that causes increasingly troublesome dysphagia (difficulty swallowing food or liquids) and chest pain over time.
Diverticulectomy is typically performed to remove esophageal diverticula, a condition of the esophagus where a pouch forms and protrudes outward in a weak portion of the esophageal lining.

Surgery for gastroesophageal reflux is gastric fundoplication which effectively reduces or eliminates reflux symptoms caused by stomach acid. Fundoplication can be performed using minimally invasive techniques and is safe and effective with long-lasting results. As with all surgical approaches, continued surveillance is needed to monitor changes in the esophagus.
Robot-assisted Surgery – A Minimally Invasive Approach
Minimally invasive approaches have revolutionized recovery from a variety of surgeries. At St. John’s, we offer Robot Assist Minimally Invasive Esophagectomy (RAMIE). The surgeon controls the robots’ instruments and viewing tools from a remote console near the patient, which involves using smaller incisions that traditional, open surgery. Our surgeons complete the necessary procedures in less time than open surgeries, and with excellent short term and long-term results. Minimally invasive surgery requires less recovery time, shorter hospital stays, and there is less pain involved.
Why is Surveillance Important?

Surveillance plays a crucial role in the management of benign esophageal diseases, particularly in cases of Barrett’s esophagus. Regular monitoring through endoscopies or imaging studies helps detect any progression to high-grade dysplasia or esophageal cancer. High-grade dysplasia may require more aggressive interventions, such as endoscopic resection, endoscopic ablative therapies, or surgical resection.
The treatment of benign esophageal diseases involves a comprehensive approach tailored to the specific condition and the patient’s needs. It includes lifestyle modifications, medications, endoscopic interventions, surgical procedures, surveillance, and management of high-grade dysplasia. At Saint John’s our gastroenterologists, surgeons, dietitians, and other healthcare professionals work in close coordination with each other and are crucial as a team to providing effective and individualized care for our patients.
With appropriate treatment, patients can experience symptom relief, improved quality of life, and a reduced risk of complications. Call today to learn more about diagnosis and treatment. Our multi-disciplinary team is ready to support you.
If you have questions about Benign Esophageal Disease and treatment options, please call today. Click here to request an appointment.