The Margie Petersen Breast Center at Saint John’s Health Center in Santa Monica, California, is a beacon of hope and care for individuals navigating breast health concerns. With a renowned team of oncologic, screening, and genetic experts, the center provides a comprehensive and compassionate approach to breast health.
Understanding and addressing high-risk breast lesions is a key focus at the Margie Petersen Breast Center, as early and accurate diagnosis is essential in reducing uncertainty and empowering patients with clear, actionable information. By identifying and managing these conditions promptly, the center equips patients with the knowledge and resources to make informed decisions about their care.
Proliferative Lesions with Atypia
These lesions, while not cancerous, indicate an increased risk of developing breast cancer. You physician should monitor these lesions and take proactive steps, which can make a significant difference in early diagnosis.
Atypical Ductal Hyperplasia (ADH)
This condition involves abnormal cell growth in the ducts, sharing some features with ductal carcinoma in situ (DCIS). Because of its nature, a surgical excisional biopsy is often recommended to check nearby tissues for any concerning changes. While ADH doesn’t present with visible external symptoms, it may appear as microcalcifications during a mammogram, allowing early detection and management.
Lobular Neoplasia (ALH and LCIS)
Including atypical lobular hyperplasia (ALH) and lobular carcinoma in situ (LCIS), these are markers of increased breast cancer risk. They are often found incidentally during imaging or biopsy, as they typically don’t cause palpable lumps or symptoms. Depending on individual cases, your healthcare provider might suggest close observation or surgical excision to ensure careful management.
Flat Epithelial Atypia (FEA)
This precancerous condition is not harmful on its own, but it is sometimes discovered alongside more worrisome lesions. For this reason, a surgical excisional biopsy is recommended. Flat epithelial atypia doesn’t cause visible or physical symptoms, making imaging and biopsy critical in its identification.

Fibroepithelial Lesions
These types of lesions originate in the connective tissue of the breast and are often detected as part of routine imaging or as palpable masses.
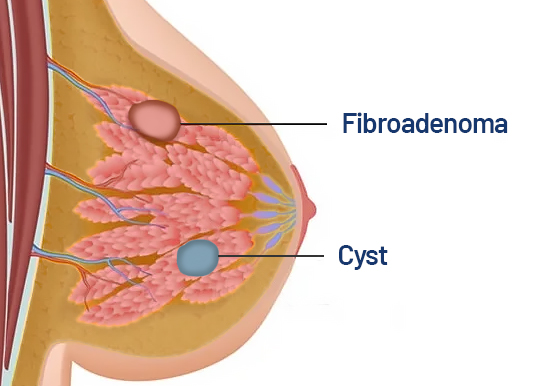
Fibroadenoma
Common and benign, fibroadenomas are firm, rubbery, and moveable masses that are often discovered during a physical exam or imaging. While most fibroadenomas don’t require removal, they can be monitored, especially if they grow or cause discomfort. Their benign nature is confirmed through biopsy, bringing peace of mind.
Phyllodes Tumors
Though rare, this tumor may resemble a fibroadenoma in feel and appearance, but it can grow more rapidly. Most phyllodes tumors are benign, but on rare occasions, they can be malignant. To ensure thorough evaluation, these tumors are excised completely. Recognizing and addressing such growths promptly can provide clarity and reassurance.
Additional High-Risk Lesions
Pseudoangiomatous Stromal Hyperplasia (PASH)
This benign condition usually presents as a firm, moveable mass that is painless. It consists of myofibroblastic cells and can be monitored unless it causes discomfort, in which case removal might be considered. Knowing it’s non-cancerous can be a relief to those concerned about a palpable lump.
Sclerosing Lesion
Typically benign, this hardened tissue can take the form of sclerosing adenosis, which involves extra growth within breast lobules. While not associated with cancer, these lesions may require follow-up imaging or biopsy to confirm their nature, offering a sense of security.

Complex Cysts
These cysts are a combination of fluid and solid material. Unlike simple fluid-filled cysts, complex cysts are aspirated to rule out malignancy. They are often diagnosed through ultrasound and can be reassuringly benign, although management provides clarity.
Radial Scar (RS)
Rare and often without symptoms, radial scars are usually found during imaging or biopsy. Due to their association with conditions like DCIS and invasive carcinoma, they are excised for further evaluation. Addressing them early helps to reduce uncertainty.
Breast Calcifications
Visible as microcalcifications on mammograms, these mineral deposits are common and often benign. However, if imaging suggests a concern, surgical excision may be recommended to rule out malignancy. Their detection during routine screenings is an important step in proactive breast health.
Other Breast Considerations
Papillomas, which are noncancerous growths within the ducts, might cause nipple discharge or present as a small lump. Fibrocystic changes, a benign and common response to hormonal fluctuations, can mimic symptoms of high-risk lesions. Finally, columnar cell changes, while typically benign, may occasionally increase cancer risk and warrant monitoring.
Please remember, you’re not alone in this journey. Early detection and the guidance of skilled healthcare professionals make a tremendous difference in staying healthy and informed. If you have any concerns or questions about these conditions, your medical team is there to provide personalized care and support.
Contact the Margie Petersen Breast Center

The Margie Petersen Breast Center at Providence Saint John’s Health Center is widely renown for its outstanding and compassionate patient care, expert surgical and medical team, and ability to fully evaluate any breast condition in one day.
Meet Our Breast Health Experts
The Breast Health Clinic can be reached at (310) 582-7209. If you have questions regarding a new symptom or want to make an appointment for evaluation please call and a staff member will assist with navigating you in the right direction.



