

Cushing’s Syndrome is a hormonal disorder caused by prolonged exposure to elevated cortisol levels. Cortisol is a hormone produced by the adrenal glands that plays an important role in metabolism, blood pressure regulation, immune response, and the body’s stress response.
At Saint John’s Health Center, our Endocrine Center of Excellence provides comprehensive evaluation and treatment for adrenal and endocrine disorders, including Cushing’s Syndrome, adrenal tumors, thyroid diseases, and inherited endocrine conditions. Our multidisciplinary endocrine specialists work closely together to identify the underlying causes and develop individualized treatment plans.
What Is Cushing’s Syndrome?
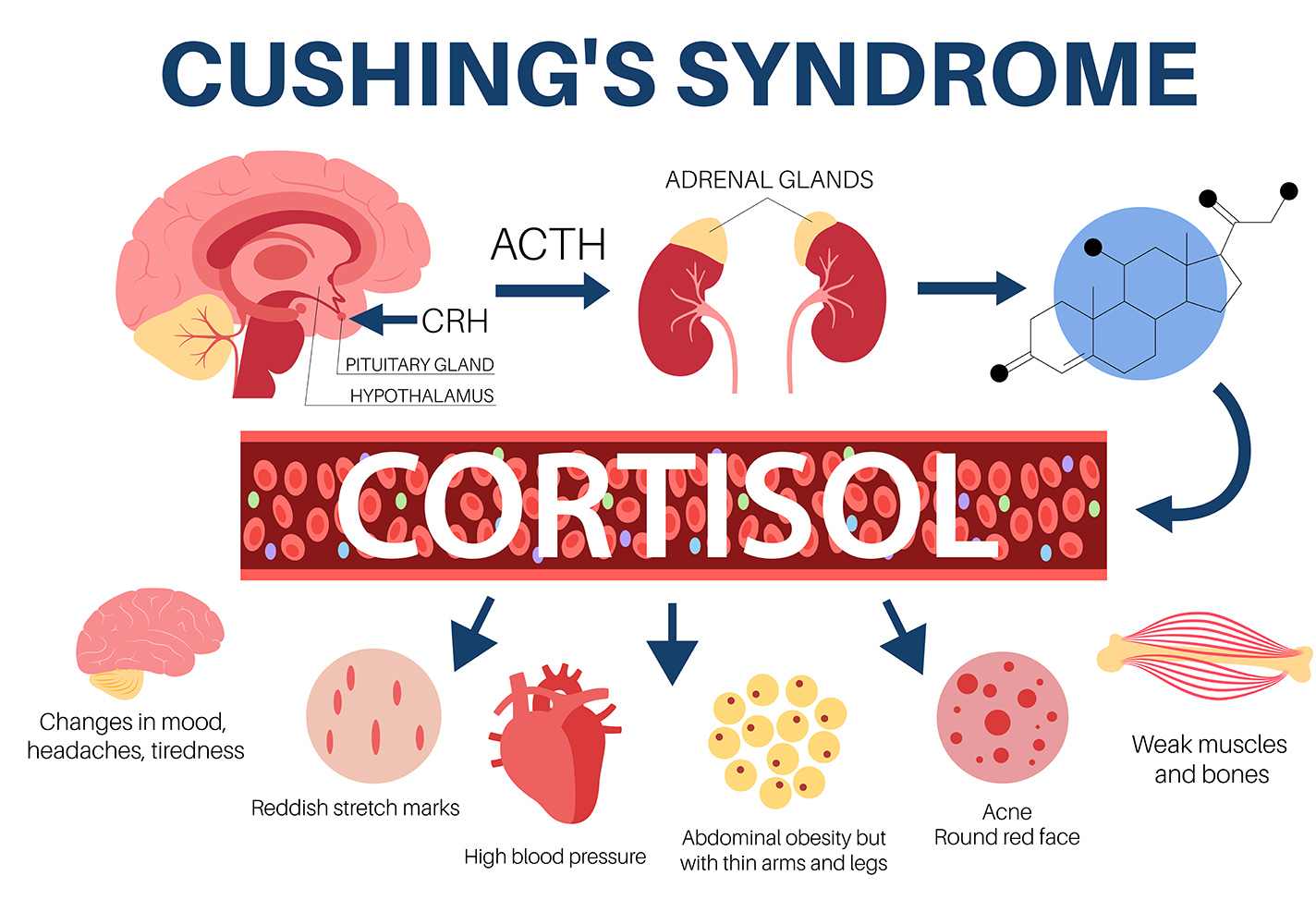
Cushing’s Syndrome occurs when the body is exposed to excessive cortisol levels over an extended period of time. Cortisol is a hormone produced by the adrenal glands that helps regulate metabolism, blood pressure, immune response, blood sugar, and the body’s reaction to physical and emotional stress. Elevated cortisol may develop because the body is producing too much cortisol internally or because of long-term corticosteroid medication use.
When cortisol levels remain abnormally elevated, multiple organ systems throughout the body can be affected. Patients may experience changes involving weight distribution, muscle strength, blood pressure, blood sugar, bone health, mood, sleep, and overall energy levels. Because symptoms often develop gradually and may overlap with more common medical conditions such as obesity, diabetes, fatigue, depression, or metabolic syndrome, diagnosis can sometimes be delayed or difficult to recognize in earlier stages.
Signs and Symptoms of Cushing’s Syndrome
The symptoms of Cushing’s Syndrome can vary widely between patients depending on the severity and duration of cortisol excess. Some patients experience noticeable physical changes, while others may present with more subtle metabolic abnormalities or only mild symptoms. Some patients may experience only mild or “subclinical” Cushing’s Syndrome with minimal outward symptoms despite abnormal laboratory findings. Even mild cortisol excess may contribute to long-term cardiovascular, metabolic, and bone-related complications if left untreated.
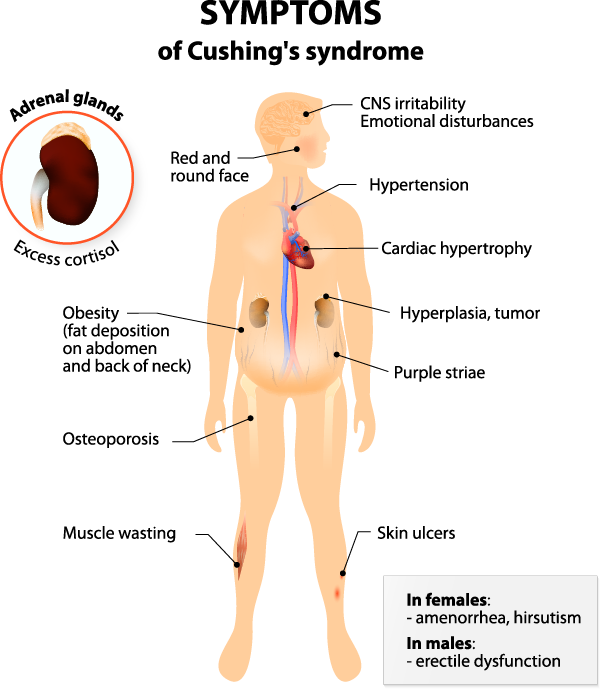
Common signs and symptoms may include:
- Weight gain, particularly around the abdomen and upper body
- Rounded facial appearance (“moon face”)
- Fat accumulation at the back of the neck (“buffalo hump”)
- Fatigue and muscle weakness
- Easy bruising and thinning skin
- Wide purple or pink stretch marks
- High blood pressure
- Elevated blood sugar or diabetes
- Osteoporosis or bone loss
- Swelling in the legs
- Irregular menstrual cycles
- Mood changes, anxiety, depression, or difficulty concentrating
Causes of Cushing’s Syndrome
Determining the source of cortisol excess is one of the most important steps in developing an effective treatment plan. Different causes of Cushing’s Syndrome require different diagnostic and treatment approaches.
Pituitary Tumors (Cushing’s Disease)
The most common cause of endogenous Cushing’s Syndrome is a pituitary tumor, often referred to as Cushing’s disease. These typically benign pituitary tumors produce excess adrenocorticotropic hormone (ACTH), which stimulates the adrenal glands to overproduce cortisol. Pituitary-related Cushing’s Syndrome accounts for the majority of endogenous cases and often requires specialized endocrine testing and imaging to confirm the diagnosis.
Adrenal Tumors

Adrenal tumors can also directly produce excess cortisol independent of ACTH regulation. These tumors may include benign adrenal adenomas, bilateral adrenal hyperplasia, or, less commonly, adrenal cancer. Because adrenal tumors bypass the body’s normal hormonal feedback mechanisms, cortisol production may remain continuously elevated. Imaging studies such as adrenal-protocol CT scans or MRI are often used to help identify adrenal causes of Cushing’s Syndrome.
Ectopic ACTH-Producing Tumors
In some cases, tumors located outside the pituitary gland may produce ACTH or ACTH-like hormones that stimulate excess cortisol production. These are known as ectopic ACTH-producing tumors and may occur in the lungs, pancreas, thymus, or other locations. Although less common, ectopic tumors can lead to severe cortisol excess and often require comprehensive endocrine evaluation and imaging studies to identify the source.
Long-Term Steroid Use
Long-term use of corticosteroid medications remains one of the most common causes of Cushing’s Syndrome overall. Steroid medications used to treat conditions such as asthma, rheumatoid arthritis, lupus, or autoimmune disease can produce symptoms similar to endogenous Cushing’s Syndrome when used over prolonged periods or at high doses. Whenever medically appropriate, physicians may gradually adjust steroid therapy to help reduce cortisol-related complications while continuing to manage the underlying condition safely.
Risk Factors for Cushing’s Syndrome
Several factors may increase the risk of developing Cushing’s Syndrome or related endocrine tumors.

Risk factors may include:
- Long-term corticosteroid medication use
- Pituitary or adrenal tumors
- Inherited endocrine tumor syndromes
- Family history of endocrine tumors
- Women between 30 and 50 years of age
- Multiple hormone-producing endocrine tumors
- Adrenal hyperplasia or adrenal nodules
Certain inherited endocrine syndromes, including Multiple Endocrine Neoplasia (MEN) and other inherited syndromes, may increase the risk of pituitary and adrenal tumors associated with cortisol excess. Patients with multiple endocrine tumors or strong family histories may benefit from genetic counseling and endocrine evaluation.
Why Cushing’s Syndrome Can Be Difficult to Diagnose
Diagnosing Cushing’s Syndrome can sometimes be challenging because many symptoms overlap with more common conditions such as obesity, diabetes, high blood pressure, fatigue, depression, or metabolic syndrome.
In some patients, symptoms develop gradually over several years, making changes more difficult to recognize early. Mild or intermittent cortisol excess may also produce abnormal laboratory findings before more obvious physical symptoms develop. Because untreated cortisol excess may increase long-term cardiovascular, metabolic, and bone-related risks, comprehensive endocrine evaluation is important even when symptoms appear mild or nonspecific.
How Cushing’s Syndrome Is Diagnosed
Diagnosis of Cushing’s Syndrome typically involves a combination of laboratory testing, clinical evaluation, and imaging studies designed to confirm elevated cortisol levels and determine the source of hormone excess. Because cortisol levels naturally fluctuate throughout the day and symptoms may overlap with more common medical conditions, diagnosis often requires careful interpretation of multiple tests rather than relying on a single laboratory result. Endocrine specialists evaluate not only cortisol levels themselves, but also how the body regulates cortisol production over time. Once elevated cortisol is confirmed, additional testing and imaging help determine whether the source is related to the pituitary gland, adrenal glands, ectopic hormone-producing tumors, or long-term corticosteroid medication use.
Hormonal Testing
Initial testing may include:
- 24-hour urinary free cortisol testing
- Late-night salivary cortisol testing
- Low-dose dexamethasone suppression testing
- Blood cortisol measurements
- ACTH testing
- Additional endocrine laboratory studies when indicated
Certain medications and medical conditions may affect cortisol testing results, so repeat testing or medication adjustments may sometimes be necessary for accurate interpretation.

and adrenal-protocol CT scan may be used to determine the source, being pituitary, adrenal, or ectopic.
Imaging Studies
Once elevated cortisol levels are confirmed, imaging studies help determine whether the source is pituitary, adrenal, or ectopic.
Imaging may include:
- Pituitary MRI
- Adrenal-protocol CT scan
- MRI of the adrenal glands
- Specialized endocrine imaging studies
In selected cases, additional testing such as inferior petrosal sinus sampling may be recommended to distinguish between pituitary and ectopic ACTH production.
Treatment and Management of Cushing’s Syndrome
Treatment depends on the underlying source of cortisol excess and the severity of symptoms. The primary goal of treatment is to normalize cortisol levels while reducing long-term complications related to metabolic, cardiovascular, and bone health.
Surgery for Cushing’s Syndrome

Surgery is often the preferred treatment for tumors causing cortisol excess.
Treatment options may include:
- Transsphenoidal surgery for pituitary tumors
- Adrenalectomy for adrenal tumors
- Surgical removal of ectopic ACTH-producing tumors
The recommended surgical approach depends on the location, size, and type of tumor identified during evaluation.
Medical Therapy
When surgery is not appropriate or additional treatment is needed, medications may help reduce cortisol production or control symptoms related to cortisol excess. Medical therapy may be considered before surgery, after surgery if cortisol levels remain elevated, when surgery is not feasible, or during long-term endocrine management. Treatment plans are individualized and carefully monitored by endocrine specialists.
Lifestyle and Long-Term Health Management
Although medical treatment is necessary to address cortisol excess, lifestyle modifications may also help support recovery and long-term health.
Patients are often encouraged to:
- Maintain a balanced diet
- Participate in appropriate physical activity
- Support bone health
- Monitor blood pressure and blood sugar
- Prioritize sleep and stress management
- Continue long-term endocrine follow-up care
Recovery After Treatment for Cushing’s Syndrome
Recovery from Cushing’s Syndrome often occurs gradually after cortisol levels normalize. Because the body adapts to prolonged cortisol excess over time, many symptoms improve slowly during the months following treatment.
Hormonal Recovery
Following successful treatment, patients may temporarily require steroid replacement medications while the body’s normal cortisol regulation recovers. Endocrinologists closely monitor hormone levels and gradually adjust medications during recovery. In some patients, hormonal recovery may take several months or longer depending on the duration and severity of cortisol excess before treatment.
Improvement in Symptoms
Many patients gradually experience improvement in weight distribution, facial swelling and rounding, blood pressure, blood sugar control, bruising and skin fragility, muscle strength, mood, concentration, and energy levels. Although some improvements may occur within weeks, complete metabolic recovery can continue for 12 to 18 months or longer in some individuals.
Long-Term Follow-Up

Some long-standing complications related to cortisol excess may require ongoing monitoring even after successful treatment. Patients with prolonged disease may continue follow-up care for:
- Diabetes or blood sugar control
- Bone density and osteoporosis
- Cardiovascular health
- Adrenal hormone recovery
- Autoimmune conditions that may re-emerge after cortisol normalization
Regular endocrine follow-up remains an important part of long-term care after treatment.
Frequently Asked Questions About Cushing’s Syndrome
Can Cushing’s Syndrome be mild or intermittent?
Yes. Some patients develop mild or “subclinical” Cushing’s Syndrome with only subtle symptoms or abnormal laboratory findings. Even mild cortisol excess may contribute to long-term health risks and should be evaluated carefully.
How long does it take to recover after treatment?
Recovery timelines vary depending on the severity and duration of cortisol excess. Some patients begin improving within weeks, while full recovery of metabolism, energy, and physical symptoms may take many months.
Can long-term steroid medications cause Cushing’s Syndrome?
Yes. Prolonged corticosteroid use remains one of the most common causes of Cushing’s Syndrome and should be carefully monitored by healthcare providers.
Will symptoms completely go away after treatment?
Many symptoms improve significantly after successful treatment, although some long-standing complications may require continued medical management and follow-up care.
Questions About Cushing’s Syndrome?
If you have questions about Cushing’s Syndrome, elevated cortisol levels, adrenal tumors, or endocrine testing, our specialists can help guide evaluation, diagnosis, treatment planning, and second opinions.
Cushing’s Syndrome care is part of the broader Endocrine Center of Excellence at Saint John’s Health Center. The endocrine specialists at Saint John’s Health Center provide comprehensive care for patients with Cushing’s Syndrome, adrenal tumors, pituitary disorders, and complex endocrine conditions. Our multidisciplinary approach combines advanced endocrine testing, imaging, surgical expertise, and long-term hormonal management tailored to each patient’s diagnosis and recovery needs.
If you have questions regarding thyroid cancer treatment or diagnosis, please call today. Click here to request an appointment.



