Personalized Care for Endocrine Tumors and Disorders
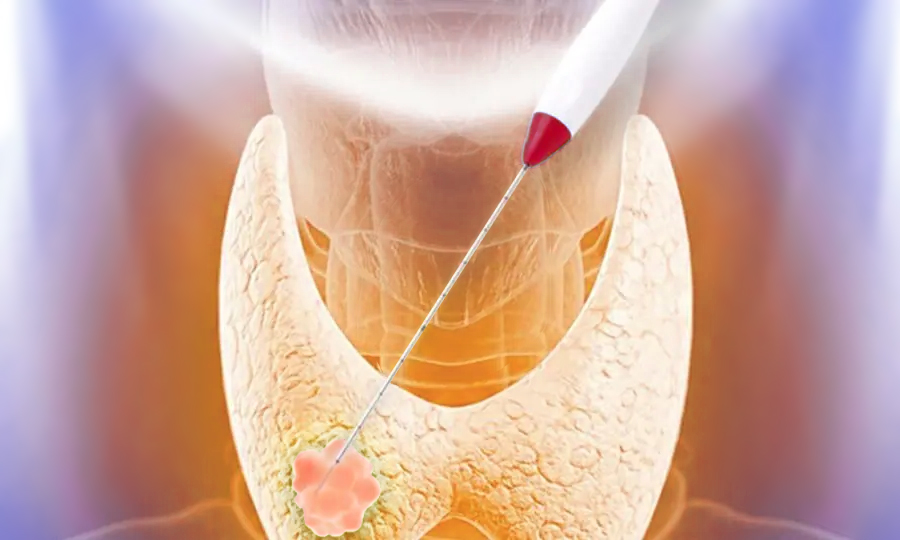
Endocrine Tumors and Disorders Center, located in Santa Monica, CA is a comprehensive, multidisciplinary clinic for patients (older, younger, adolescents and adults) with endocrine conditions. Watch our video to learn about the Endocrine Tumors and Disorders center approach to care for patients with diabetes, thyroid disease, thyroid cancer, adrenal masses, adrenal cancer and other endocrine conditions.
Dr. Melanie Goldfarb, Dr. Sarah Rettinger, and Dr. Frederick Singer describe their multidisciplinary approach to thyroid and endocrine care.