Mediastinal Tumor cases are reviewed by a multi-disciplinary tumor board at Saint John’s Cancer Institute and Health Center to personalize effective treatment plans.
What is the Mediastinum?
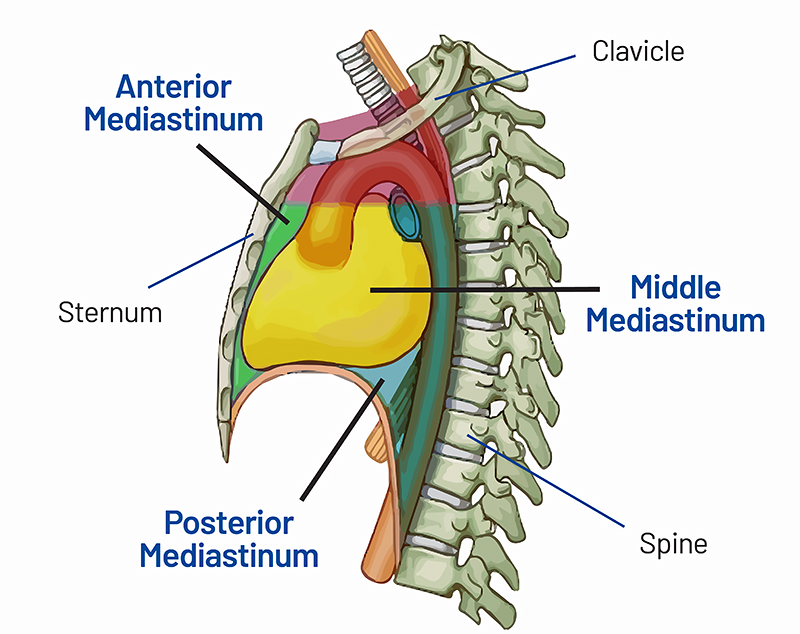
The mediastinum is an anatomic space occupying the cavities that exist between the lungs and the chest. The top of the mediastinum has discrete boundaries which are separated from the neck by the bones of the sternum, upper ribs, spine, and clavicle. Below the mediastinum cavity from the abdomen is the muscle used for breathing, called the diaphragm. On either side of the mediastinum are the right and left lungs.
The mediastinum is divided into 3 parts: the anterior (front), middle, and posterior section (back).
The Anterior (Front) Mediastinum:
The anterior section is in front of the heart, bordered by the breastbone, or sternum. As children this space is large and well-formed and contains fat and tissue from an organ called the thymus, which served as an immune function. As adults this space is smaller, and the function of the thymus is transferred to the spleen, liver, and bone marrow. With time, the thymus disappears all together, leaving an unoccupied space called, the anterior mediastinum, where a tumor can form.

The most frequent place that we see abnormalities in the mediastinum is in the anterior mediastinum. Several tumors and abnormalities can develop in this space. Most commonly, abnormalities of the thymus gland including, thymoma tumors or thymic cysts.
A few other growths can also present in the anterior mediastinum. Such as lymphomas, which are tumors of a lymph node origin, and teratomas or germ cell tumors, which are tumors of very basic elements from our cells. Nearby organs, such as the thyroid gland, can also expand into the anterior mediastinum. Many of these tumors are relatively indolent and slow growing, having a benign nature. More aggressive cancers of the anterior mediastinum include thymic carcinomas and aggressive lymphomas.
Thymoma
The most common anterior mass is a thymoma. There are different types of thymomas. They are generally seen on CT as a round, encapsulated mass, and rarely recur. The larger irregular masses, malignant thymic carcinomas are much more aggressive and have a much worse prognosis.
Lymphoma
is a cancer that arises in cancer-fighting cells called lymphocytes. Lymphoma usually starts in lymph nodes, the spleen, or the bone marrow. Infrequently, lymphoma starts in the anterior mediastinum. There are 2 categories of lymphoma: Hodgkin’s disease and non-Hodgkin’s lymphoma.
Germ Cell
A rare mediastinal mass is a germ cell a tumor. They are very rare. They are usually benign (60 to 70%) and are found in both males and females.
Thyroid Mass
substernal goiter remains a significant consideration in the differential diagnosis of mediastinal masses, particularly those located in the anterior mediastinum. Substernal goiter is generally defined as a thyroid mass that has 50% or more of its volume located below the thoracic inlet.
The Middle Mediastinum
The middle section of the mediastinum contains organs such as the windpipe (better known as the trachea), the heart, as well as the aorta and other great vessels that go to the heart. Tumors can develop in the middle section of the mediastinum.
Bronchogenic Cyst
Bronchogenic cysts are congenital in nature. They are part of a spectrum of congenital abnormalities of the lung, including pulmonary sequestration, congenital cystic adenomatoid malformation, and congenital lobar hyperinflation (emphysema)
Pericardial Cysts
Pericardial cysts are an uncommon benign congenital anomaly in the middle mediastinum. They represent 6% of mediastinal masses, and 33% of mediastinal cysts.
There are several benign cystic lesions that can develop in the middle and posterior mediastinum. These include cysts associated both with the airway, as well as the esophagus the muscular tube that connects the mouth to the stomach. The cysts are generally congenital in nature and can grow over the course of time. Very rarely these cysts can degenerate into infections or cancers. In general, when these cysts are detected, doctors recommend removal.
The Posterior Mediastinum
The posterior mediastinum is located behind the heart and is bound by the spine. This space contains blood vessels, nerves, and the esophagus. Tumors can develop in the posterior section of the mediastinum.
Neurogenic Tumors
The most common cause posterior mediastinal tumors arise from nerves. They are usually benign, especially in adults. They are usually on the side of the backbone.
Symptoms of Mediastinal Tumors

In general, mediastinal tumors are rare. They occur in patients aged 30 to 50 years. In children, tumors are most often found in the posterior (back) mediastinum, arising from the nerves. These mediastinal tumors are typically benign (not cancer). Most are found when a chest x-ray is performed for another reason.
- Cough
- Shortness of breath
- Wheezing
- Chest pain or fullness
- Fever
- Chills
- Night sweats
- Coughing up blood
- Hoarseness
- Weight loss
Diagnosis of Mediastinal Tumors
Frequently, surgeons are asked to obtain adequate tissue to diagnose the nature of mediastinal tumors.
However, mediastinal tumors may not require a biopsy because they demonstrate characteristic CT or MRI finding that obviate the need for a biopsy. This is certainly the case with thymomas or cystic lesions of the middle portion of the mediastinum. Germ cell tumors, or teratomas, have characteristic findings on a CT that do not require a biopsy prior to intervention either. Tumor proximity and risk to other anatomical structures, such as the thyroid gland, may prevent a biopsy in the mediastinum as well.
The tests most used to diagnose and evaluate a mediastinal tumor include:
Blood Tests
Blood tests may include, Alpha feto protein (AFP), beta HCG, and LDH
Tissue Biopsy
CT-guided needle biopsy
May make the diagnosis.
Mediastinoscopy
Provides a sample of the tissue for the middle mediastinum. Does not help with posterior or anterior mediastinum. This is an outpatient procedure under general anesthesia done through a 1-inch incision in the neck.
Anterior mediastinotomy (Chamberlain procedure)
Just beside the sternum, an incision is made in the chest to get a piece of tissue from the mass.
EBUS (EndoBronchial UltraSound)
This is an outpatient procedure done without incisions. The tissue is obtained with a needle aspiration so only a small amount of tissue can be obtained so often enough tissue in not obtained through with a procedure.
The choice of test for diagnosis depends on the appearance on the CT scan. If an anterior mediastinal mass looks like a thymoma, the mass is usually resected if it does not look to be invading surrounding body parts. If an anterior mediastinal mass looks like lymphoma, the biopsy approach is mediastinoscopy (if nodes look involved) or anterior mediastinotomy if there is an anterior mediastinal mass and if the nodes look normal.
Imaging Tests For Mediastinal Tumors

Chest X-Ray
May not provide a discrete boundary for mediastinal tumors but leads to further testing.
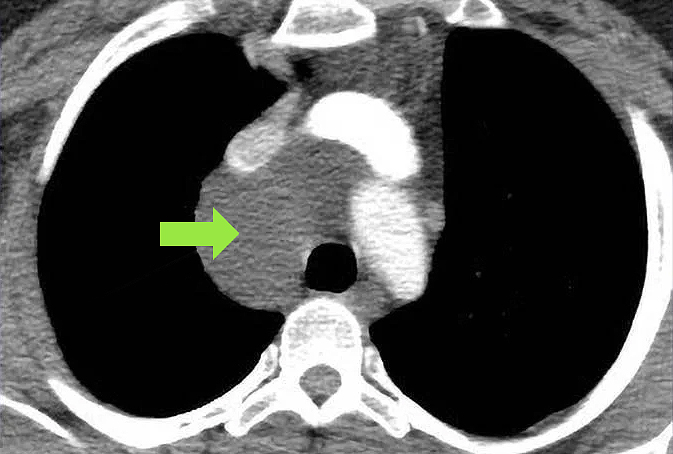
Computed Tomography (CT)
This chest scan provides the appearance of the mass which may suggest what the diagnosis is.
Magnetic Resonance Imaging (MRI)
May help define the relationship of mediastinal masses.
Stages of Mediastinal Cancer
Stage Definition
Staging is defined by tumor size, location of cancer, and how far the cancer spread to other parts of the body.
- I Macroscopically and Microscopically Completely Encapsulated: Noninvasive cancer encapsulated.
- IIA Microscopic Trans Capsular Invasion: Cancer growing into the capsulated area.
- IIB Macroscopic Invasion: Cancer growing outside the capsule into surrounding fatty tissue or grossly adherent to but not through mediastinal pleura or pericardium.
- III Macroscopic Invasion: Cancer spreading to nearby organs or tissue. Which include the sac surrounding the heart, the lungs, and main blood vessels to the heart.
- IVA Pleural or Pericardial Dissemination: Widespread cancer throughout the heart and lungs.
- IVB Lymphogenous or Hematogenous Metastasis: Cancer has metastasized to other body parts. Such as liver, lungs, and bones.
If you have questions regarding Mediastinal Tumors and Treatment, please call today. Click here to request an appointment.



