
The treatment of emphysema requires an expert surgical approach. At Saint John’s Health Center, our thoracic surgeons are internationally recognized and have contributed to the development of surgical treatments for emphysema, writing over 100 peer-reviewed journal articles.
Emphysema is a progressive disease that can compromise the quality of life for people with severe conditions. Because medical management has provided minimal impact on the disease, a variety of surgical procedures can improve outcomes. The most effective operation has been lung volume reduction surgery (LVRS).
What is Lung Volume Reduction Surgery? (LVRS)
Lung Volume Reduction Surgery (LVRS) is a surgical procedure designed to alleviate the symptoms and improve the quality of life for patients suffering from severe emphysema, a progressive lung disease primarily caused by smoking and characterized by the destruction of lung tissue. Emphysema leads to reduced lung function and breathing difficulty. LVRS tratment aims to decrease the size of hyper-inflated lungs, allowing the remaining healthier lung tissue to function more efficiently. Comprehensive evaluations, including Pulmonary function tests (PFTs), chest imaging, and overall health assessments, are vital in determining the suitability of candidates for LVRS treatment.
How does LVRS help with severe emphysema?
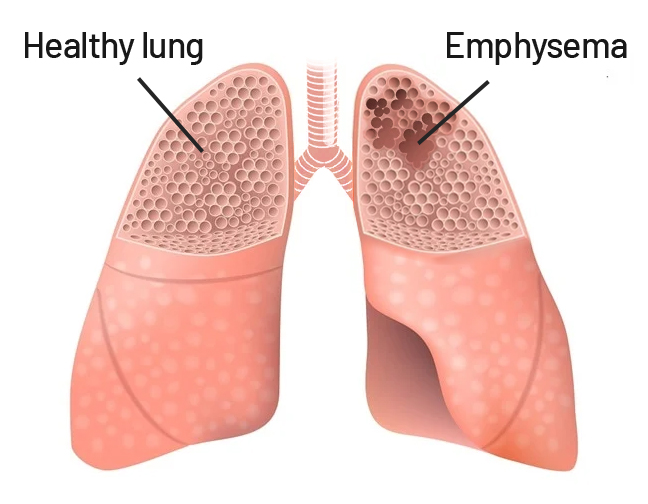
Emphysema is characterized by the loss of elasticity in the lung tissue, leading to air becoming trapped in the alveoli (air sacs), and causing hyperinflation. This condition results in impaired oxygen exchange and increased work breathing. Individuals with severe emphysema often experience symptoms such as shortness of breath, chronic cough, wheezing, fatigue, and reduced exercise tolerance. As the disease progresses, these symptoms can become debilitating and significantly impact the patient’s well-being.
The decision to undergo LVRS is usually considered when conservative treatments such as medication, pulmonary rehabilitation, and oxygen therapy have not provided sufficient relief. Patients with severe emphysema who meet certain criteria, such as having low exercise capacity and significant hyperinflation, are potential candidates for LVRS. Before proceeding with the surgery, patients typically undergo a thorough evaluation, including pulmonary function tests (PFTs), imaging studies (such as chest CT scans), and assessments of overall health. The average length of stay in the hospital is 7 days.
Benefits of LVRS Treatment
LVRS primarily involves removing the upper lobes. By reducing the size of the over-inflated lung, the remaining lung tissue is allowed to expand more effectively, leading to improved ventilation and gas exchange. The surgery can be performed either through traditional open surgery or minimally invasive techniques such as video-assisted thoracoscopic surgery (VATS).
While LVRS can bring substantial benefits to patients with severe emphysema, it’s important to note that like any major surgical procedure, it carries risks. Potential complications include infection, bleeding, respiratory failure, and even death, although these risks are greatly minimized with advancements minimally invasive surgical techniques and patient selection criteria.
What are the Indications for LVRS?
Patients who are symptomatic despite maximal medical management for severe emphysema are candidates for LVRS. Their symptoms usually include shortness of breath with everyday activities including showering, carrying, walking short distances, and bending.
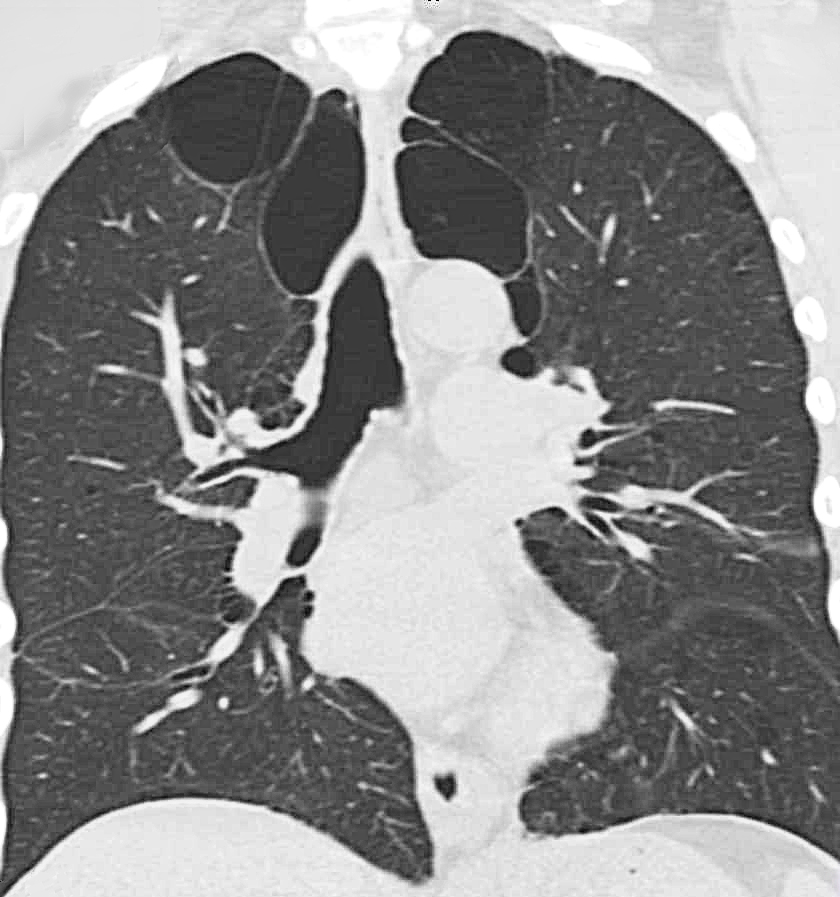
Imaging scans will tend to reveal hyper-inflated lungs with a depressed diaphragm. A CT scan may show a heterogeneous pattern of emphysema in the lungs, which is generally much worse in the upper lobes of the lung than in the lower lobes. This is usually confirmed with a lung perfusion scan.
What can I expect After LVRS treatment?
After LVRS treatment, many patients experience significant improvements in their quality of life. Studies have shown that up to 75% of patients who required supplemental oxygen before the surgery no longer need it after recovery. Improved exercise tolerance, reduced shortness of breath, and enhanced overall functioning are among the positive outcomes observed in many cases. However, it’s crucial to emphasize that patient selection is critical to achieving these positive results.
For patients who might be unsure about undergoing surgery or do not meet the criteria for LVRS, clinical trials may offer an alternative approach. These trials investigate new treatments, medications, or interventions that could potentially benefit individuals with severe emphysema. Participation in clinical trials helps to advance medical knowledge and improve treatment options for patients.
Call today to learn more about emphysema treatment and symptoms. Our multi-disciplinary team is ready to support you.
If you have questions regarding LVRS Treatment, or Emphysema symptoms, please call today. Click here to request an appointment.



